INTRODUCTION
Gallstone ileus is a relatively rare condition, occurring in 0.30.5% of individuals with cholelithiasis, resulting from the impaction of a gallstone in the gastrointestinal tract, typically in the terminal ileum. It accounts for approximately 1-4% of all cases of intestinal obstruction1. Diagnosis can be challenging due to an atypical symptom profile, necessitating a high level of clinical suspicion for prompt identification. As a result, it is often diagnosed only during surgery, resulting in a significant risk of morbidity and mortality 1,2.
Approximately half of the affected individuals have a prior history of gallstone disease. While around 4% of patients under the age of 65 experience bowel obstruction due to gallstone ileus, this rate rises to as high as 25% in patients aged 65 and older [3]. The inflammation and pressure exerted by the gallstone can erode the gallbladder wall, leading to the formation of a fistula between the gallbladder and the gastrointestinal tract, most commonly involving the duodenum. The most common site for the development of a cholecysto-enteric fistula is from the fundus of the gallbladder to the duodenum. Given its acute onset, appropriate management strategies need to be adopted 4.
CASE REPORT
A 68-year-old man, with a history of hypertension, presented with abdominal pain, vomiting, and constipation persisting for 8 days, with constipation occurring over the last 1 day. The abdominal pain was diffuse, gradual in onset, ranged from mild to moderate in severity, and was characterized by a dull, aching sensation. The pain worsened after meals but did not radiate to the back. Oral analgesics provided partial relief. He also reported experiencing 2-3 episodes of bilious vomiting daily for the past 8 days, which was partially alleviated by medication. The patient had experienced similar symptoms in the past.
On physical examination, he exhibited generalized abdominal distension and tenderness around the umbilical area, with no signs of peritonitis. Based on these findings, he underwent a contrast-enhanced computed tomography (CT) scan of the abdomen, which revealed pneumobilia, dilated bowel loops, and gallstones in the terminal ileum (Figure 1). A diagnosis of subacute intestinal obstruction secondary to gallstone ileus was established. He was subsequently scheduled for an emergency exploratory laparotomy. Intra-operatively, two stones measuring 2.5x2.5 cm and 2x2cm were present 4 cm proximal to ileocaecal junction (Figure 2). Cholecysto-duodenal fistula was identified and a loop ileostomy done. Patient had no complications in the post-operative period and was discharged on post-operative day 3.
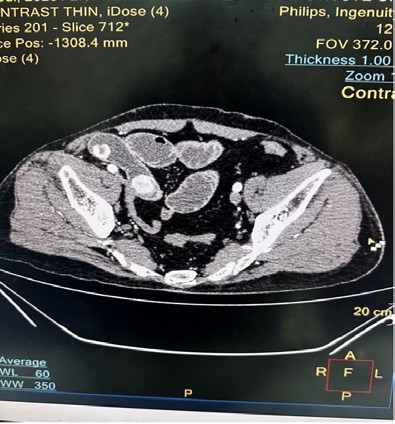
Figure 1. CECT abdomen revealing gall stones in the terminal ileum

Figure 2. Intra-operative finding of 2 gall stones in the terminal ileum.
DISCUSSION
Gall stone ileus is an uncommon condition that occurs due to erosion of the gall bladder resulting in the presence of gallstones in the intestines. This creates a spontaneous fistula (biliary enteric fistula), mostly in the duodenum 5.
Among all cases of gallstone disease, incidence of gall stone ileus is 0.3-0.5 %. 2. Rate of complications in gallstone ileus remains high, ranging from 12% to 27%, due to presence of atypical symptoms, non-specific biochemical markers, age of the patient, presence of co-morbidities, late presentation, and delayed
diagnosis 6,7.
An abdominal X-ray can reveal a specific set of signs indicative of gallstone ileus, known as Rigler’s triad. This triad includes pneumobilia, small bowel obstruction, and the presence of a gallstone 7. However, computed tomography (CT) is the preferred imaging method due to its higher sensitivity of 93% 8. Additionally, gallstone ileus may be identified intraoperatively when a patient is undergoing laparotomy for an unknown cause of small bowel obstruction 9.
Currently, two primary treatment approaches are available for gallstone ileus: the single-stage and two-stage procedures. The single-stage procedure involves a combined entero-lithotomy, cholecystectomy, and fistula closure. Conversely, the two-stage procedure starts with an entero-lithotomy and cholecystectomy, followed by fistula closure at a later stage 10. The location of the gallstone is crucial in determining the appropriate surgical approach. For gallstones lodged in the small intestine, a twostage procedure is recommended, while a one-stage procedure is preferred for gallstones in other bowel regions 11. Nonetheless, the patient’s overall health and existing medical conditions can influence surgical outcomes and should be carefully considered, particularly for single-stage procedures 5, 9. With a two-stage approach, there’s a slight risk of gallstone ileus recurrence, with approximately 10% of patients requiring additional surgical intervention 12.
ACKNOWLEDGEMENT
We are grateful to the patient and their relatives who were very co-operative during the assessment, surgery and follow up.
REFERENCES
1. Chou JW, Hsu CH, Liao KF, Lai HS, Cheng KS, Peng CY, et al. Gallstone ileus: report of two cases and review of the literature. World J Gastroenterol. 2007; 13(8):1295–98 [PubMed | Full Text | DOI]
2. Clavien PA, Richon J, Burgan S, Rohner A. Gallstone ileus. Br J Surg. 1990; 77(7):737–42. [PubMed | Full Text | DOI]
3. Palma GDD, Mastrobuoni G, Benassai G. Gallstone ileus: endoscopic removal of a gallstone obstructing the lower ileum. Dig Liver Dis. 2009; 41(6): 446. [PubMed | Full Text | DOI]
4. Kumar N, Anjum R, Mani R, Karki B. Neglected gallstone disease presented as gallstone ileus: a rare cause of intestinal obstruction. Cureus. 2021, 13(9):e18205 [PubMed | Full Text | DOI]
5. Alnahari DI, Almalki SA, Alabeidi FA. Recurrent intestinal obstruction due to gallstone ileus during same hospital admission: a case report and literature review. J Surg Case Rep. 2021(4):rjab024. [PubMed | Full Text | DOI] 6. Inukai K: Gallstone ileus: a review. BMJ Open Gastroenterol. 2019; 6(1):e000344. [PubMed | Full Text | DOI]
7. Turner AR, Sharma B, Mukherjee S. Gallstone ileus. In StatPearls [Internet]. StatPearls Publishing, Treasure Island, FL. 2021. [PubMed | Full Text ]
8. Ploneda-Valencia CF, Gallo-Morales M, Rinchon C, Navarro-Muñiz E, Bautista-López CA, Cerda-Trujillo LF, et al. Gallstone ileus: An overview of the literature. Rev Gastroenterol Mex. 2017; 82(3):248-54. [PubMed | Full Text | DOI]
9. Mishan M, Mehdikhani B. The Diagnosis and Management of Recurrent Gallstone Ileus: A Case Report. Cureus. 2022; 14(8): e27978. [PubMed | Full Text | DOI]
10. Gil LB, Miguel TF, Perea J. Rigler triad in gallstone ileus. Rev Esp Enferm Dig. 2016; 108(9):581-2.[PubMed | Full Text]
11. Jakubauskas M, Luksaite R, Sileikis A, Strupas K, Poskus T: Gallstone ileus: management and clinical outcomes. Medicina (Kaunas). 2019; 55(9):598. [PubMed | Full Text | DOI]
12. Ravikumar R, Williams JG. The operative management of gallstone ileus. Ann R Coll Surg Engl. 2010; 92(4):279-81. [PubMed | Full Text | DOI]