CASE REPORT
https://doi.org/10.47811/bhj.178
A case of apraxia of eyelid opening associated with benign essential blepharospasm in Bhutan
Samten Dorji1, Phuntsho Dorji1, Mendu Dukpa1
1Department of Ophthalmology, Jigme Dorji Wangchuck National Referral Hospital
Corresponding author:
Samten Dorji
samtend@jdwnrh.gov.bt
ABSTRACT
Apraxia of eyelid opening (AEO) is a non-paralytic motor abnormality characterized by difficulty in eyelid opening bilaterally. This is due to the inability of voluntary opening of the eyes in the absence of visible contraction of the orbicularis oculi despite sustained willful frontalis contraction. We present you a case of a 60-year-old woman with AEO associated with benign essential blepharospasm who suffered marked limitation in daily activities due to functional blindness. She was treated with botulinum toxin type A injections following which she had adequate eyelid opening in both eyes during 1 week follow up. It is essential for physicians and patients to be aware of this condition for proper diagnosis and treatment.
Keywords: Blepharospasm; Oculoplasty; Ophthalmology.
INTRODUCTION
Apraxia of eyelid opening (AEO) is a non-paralytic motor abnormality characterized by difficulty in eyelid opening bilaterally. There is an inability to voluntary open the eyes in the absence of visible contraction of the orbicularis oculi despite sustained willful frontalis contraction. Most literature recognizes AEO as a distinct clnical entity. However, it also manifests in association with a range of other neurological disorders including benign essential blepharospasm (BEB)1. It is more common in women, with a peak age of onset in the sixth and seventh decades of life2.
AEO can cause disability due to impairment in visual integrity limiting performances of activities of daily living2. In Bhutan, the awareness of this kind of condition is very poor, even among health workers. In this report, we present a case of a 60-year-old woman who presented to our clinic with AEO.
CASE REPORT
A 60-year-old female presented to the National Eye Center in Thimphu with inability to open her eyelids for a duration of 3 months. She is a housewife primarily engaged in household activities and care giving responsibility. Over these 3 months, she was unable to perform basic daily tasks due to total loss of visual function with AEO. She had no history of diurnal variation or fatiguability. She did not have a past history of ocular or neurological conditions. Prior to presenting to the ophthalmology clinic in May 2023, she had undergone medical and psychiatry evaluation for her morbidity and was found unremarkable.
On examination in the ophthalmology clinic, she was unable to open her eyelids (Figure 1A). She had bilateral upper eyelid dermatochalasis and spasms of orbicularis, procerus and corrugator muscles were noted. Upon assisted opening of eyelids, her visual acuity was 6/6 in both eyes. Intraocular pressure measured with Goldmann applanation tonometry was 10 mmHg in the right eye 12mmHg in the left eye. Extraocular muscle movements were full and free in all directions. The anterior segment and fundus evaluation in both eyes were within normal limits. General examination did not reveal any abnormality or contributary clinical findings. A comprehensive neurological evaluation revealed normal mental function, normal cranial nerve functions, absence of cerebellar signs and involuntary movements. She was referred to the medical internist to rule out any neurological disorder. A magnetic resonance imaging of the brain was done, which was unremarkable. Given the unremarkable medical and psychiatry evaluation, a diagnosis of bilateral AEO associated with BEB was made.
After providing a detailed explanation of the condition and the therapeutic option of botulinum neurotoxin type A (BoNT-A) injections, the patient gave a written informed consent to proceed with treatment. She received BoNT-A injections at seven periocular sites around each eye, along with an additional injection in the procerus muscle. Each injection site received a dose of 2.5 units of BoNT-A. She was also prescribed ocular lubricants for both eyes. At her week 1 follow up, she was able to open her eyes normally and reported that she had resumed her basic daily activities (Figure 1B). She was informed about the temporary effects of the treatment and the need for periodic repeated injections. Currently, she is being followed up 3 monthly for repeat BoNT-A injections.

Figure 1A. Photo of the patient on the first presentation, where the patient is unable to open her eyelids.
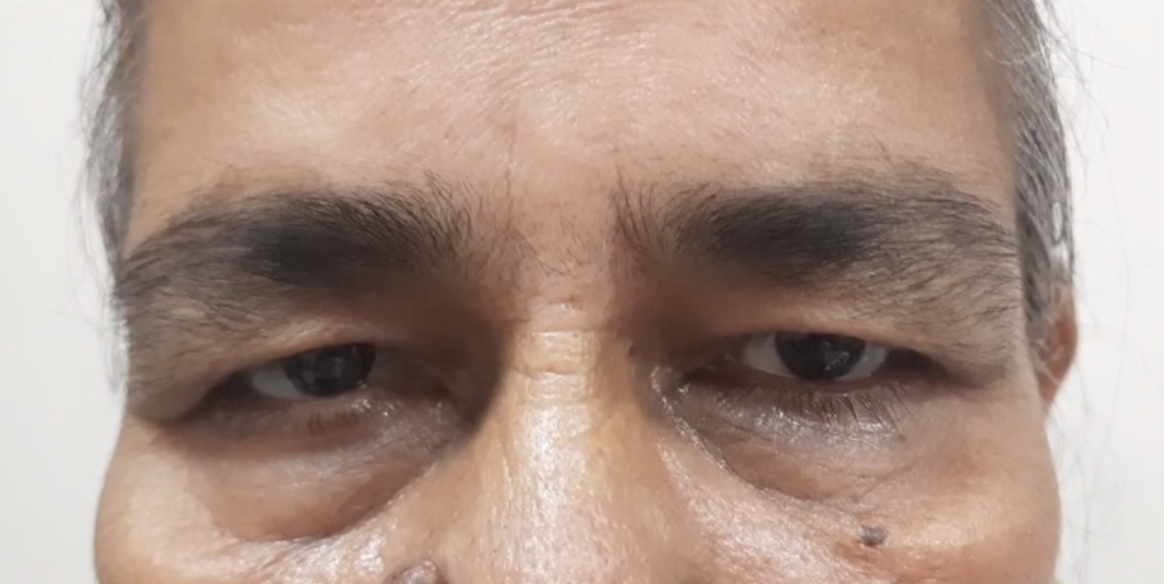
Figure 1B. Photo of the patient during week-1 follow up after botulinum toxin injection, demonstrating adequate bilateral eyelid opening
DISCUSSION
Apraxia is the inability to execute movements. In the context of AEO, it is the inability of eyelids to open. In the case that we report, AEO is associated with blepharospasm. While the pathogenesis of AEO and blepharospasm is poorly understood, few hypotheses suggest that the nigro-striatal basal ganglia pathways may project to the premotor control of eyelid coordination. Therefore, it is associated with dysfunction in the corticothalamic, basal ganglia, and focal cranial nerve circuitry3. Case reports of isolated AEO exist without blepharospasm2. Two such cases of isolated AEO associated with basal ganglia disease showed improvement following treatment with levodopa4. In patients with essential blepharospasm, the combination of spastic closure of the eyelids and levator palpebrae superioris inhibition cause difficulty with opening the lids after forced closure5.
BEB presentations can vary from mild symptoms such as increased blinking rate to functional blindness, the latter of which was present in our patient. Therefore, a clinical history is important to determine nature of the eyelid spasm. Usually, the patients will complain of bilateral, synchronous, stereotypical spasms of the orbicularis oculi muscle6.
The treatment of essential blepharospasm with botulinum toxin is well established7. It acts by inhibiting acetylcholine release at the neuromuscular junction, which leads to decreased muscle contraction. In a study done in Islamabad,1.5 to 2.0 units of BoNT-A injected at 5-7 sites over each periocular region was effective in controlling BEB8. In our case, the patient demonstrated a favourable response to BoNT-A, with 2.5 units administered at seven periocular sites around each eye along with an additional inection in the procerus muscle. This treatment was effective as the patient's AEO was associated with blepharospasm. Although BoNT-A is well tolerated, severe disease can be resistant to BoNT treatment sometimes9. Myectomy is an option when the patient fails to respond to BoNT, but the surgical procedure can have complications including post operative swelling and ecchymosis, damage to the supraorbital nerves and exposure keratopathy10. Another option is frontalis suspension surgery which has been proven to be effective and less invasive than myomectomy in combination with BoNT11.
Although we excluded other neurological conditions associated with AEO, the absence of a neurologist in our facility limited the ability to confirm the diagnosis through a more comprehensive differential exclusion, which could have strengthened the diagnostic accuracy.
Patients with this condition will have marked limitation in daily activities as it can cause functional blindness2. AEO is a diagnosis by exclusion which needs a multidisciplinary team of health personnel including neurologists, ophthalmologists and radiologists.
This case represents the first reported instance of AEO in our country. Due to the limited awareness of this condition, the patient experienced a delay in receiving appropriate management. Therefore, increasing awareness among healthcare professionals and patients is critical for the timely diagnosis and effective treatment of this condition.
ACKNOWLEDGEMENT
Department of Ophthalmology, Jigme Dorji Wangchuck National Referral Hospital
REFERENCES
1. Cabrero FR, De Jesus O. Apraxia of Lid Opening. StatPearls [Internet]. 2024 Apr 21. [Full Text]
2. Defazio G, Livrea P, Lamberti P, De Salvia R, Laddomada G, Giorelli M, et al. Isolated So-Called Apraxia of Eyelid Opening: Report of 10 Cases and a Review of the Literature. Eur Neurol. 1998;39(4):204-10. [PubMed][DOI]
3. Weiss D, Wächter T, Breit S, Jacob SN, Pomper JK, Asmus F, et al. Involuntary eyelid closure after STN-DBS: evidence for different pathophysiological entities. J Neurol Neurosurg Psychiatry. 2010;81(9):1002-7. [PubMed] [DOI]
4. Dewey RB Jr, Maraganore DM. Isolated eyelid-opening apraxia: report of a new levodopa-responsive syndrome. Neurology. 1994 Sep 1;44(9):1752-4. [PubMed] [DOI]
5. Boghen D. Apraxia of lid opening: a review. Neurology. 1997 Jun;48(6):1491-4. [DOI]
6. Titi-Lartey OA, Patel BC. Benign Essential Blepharospasm. StatPearls [Internet]. 2023 August 7. [PubMed] [Full Text]
7. Nüssgens Z, Roggenkämper P. Long-term treatment of blepharospasm with botulinum toxin type A. Ger J Ophthalmol. 1995 Nov;4(6):363-7. [PubMed]
8. Anwar MS, Zafar H. Efficacy of botulinum toxin in benign essential Blepharospasm: Desirable & undesirable effects. Pak J Med Sci. 2013 Nov-Dec; 29(6):1389-93. [PubMed] [Full Text] [DOI]
9. Jordan DR, Patrinely JR, Anderson RL, Thiese SM. Essential blepharospasm and related dystonias. Surv Ophthalmol. 1989 Sep-Oct;34(2):123-32. [PubMed] [DOI]
10. Pariseau B, Worley MW, Anderson RL. Myectomy for blepharospasm 2013. Curr Opin Ophthalmol. 2013 Sep; 24(5):488-93. [PubMed] [DOI]
11. Dressler D, Karapantzou C, Rohrbach S, Schneider S, Laskawi R. Frontalis suspension surgery to treat patients with essential blepharospasm and apraxia of eyelid opening -technique and results. Head Face Med. 2014 Oct 22;10:44. [PubMed] [Full Text] [DOI]
|
AUTHORS CONTRIBUTION Following authors have made substantial contributions to the manuscript as under: SD: Concept, design, manuscript writing, editing and review. PD: Concept, design, manuscript writing, editing and review. MD: Concept, design, manuscript writing, editing and review. Authors agree to be accountable for all respects of the work in ensuring that questions related to the accuracy and integrity of any part of the work are appropriately investigated and resolved.
|
|
CONFLICT OF INTEREST None GRANT SUPPORT AND FINANCIAL DISCLOSURE None |